
Plumbing and black nodes
February 26, 2008 § 5 Comments

Postponing is always a factor in my work. Operations are rescheduled all the time for various reasons. Last week I had prepared to film a major amputation, but ended up in the stomach and groin instead.
On this particular day I was originally going to film a hemipelvectomy (or transpelvic amputation, if you like). I’d spent some of the previous day reading up on the subject and was well prepared. Only to find out the next morning that the operation was postponed. The patient had gotten a venous thrombosis and was in no condition for this radical surgery. Must be tough on the patient. He’d probably had some hard nights of mental preparation.
So no amputation, but incidentally a total gastrectomy was on. Ventricle surgery is seldom done at my hospital. It’s a cancer center, and gastrectomies is common enough to be performed mainly at smaller community hospitals. But a video of a total gastrectomy was needed, and I’ve been waiting for a solution for some time, even considering contacting another hospital. The local hospital was hesitant to operate on this patient for some reason. They would only agree to do the pre-op chemo. By chance I’d read a blog post about ventricle surgery the night before, so at least I felt a bit prepared.
Total gastrectomy
The patient had a large tumor in the upper part of the stomach, close to the cardia. The tumor had also grown very close to the spleen, so that would have to go too, together with the entire stomach.
The first part of the operation was pretty straight forward. The blood supply and nerves of the stomach was cut. Using an instrument called GIA, which places two double rows of staples and cuts between them in one move, the duodenum and stomach was divided below the pylorus. The esophagus was separated from the stomach the same way. The spleen was then dissected and the operation specimen was removed.
The second part took a little more thinking on my part before I understood the plumbing. No disrespect to the gastrointestinal surgeons, but this really was advanced plumbing. OK. Remember that both the esophagus and the upper part of the duodenum is closed. One could think that these ends were going to be joined together, but no. Most of the gastric juices enter the small intestine in the duodenum from the pancreatic duct and the common bile duct. If the duodenum was connected directly to the esophagus, bile could enter the esophagus and cause problems. So another solution has to be found.
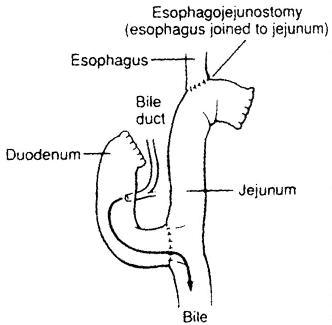
First the surgeons separated the lower part of the duodenum from the jejunum with the GIA, sealing both ends. Then they made an anastomosis between the esophagus and the jejunum 40 cm below the ligament of Treitz. Finally they made an anastomosis between the bottom part of the duodenum and the jejunum 40 cm below the first anastomosis. The upper part of the duodenum was left closed. So the food would go directly from the esophagus to the jejunum, and join with the gastric juices from the duodenum after 40 cm. The surgeons explained it to me as they were working, but I didn’t really get it until I looked up an illustration in a book the next day (photo credit). Advanced plumbing indeed.
Inguinal lymph node dissection (lymphadenectomy)
After the gastrectomy I had just enough time to wash and disinfect my equipment before the next operation started. A patient with melanoma with lymph node metastasis was going to have all the superficial nodes in his left groin removed. Again no disrespect to anyone, but this is not a very interesting operation. Lymph nodes and fat are dissected and removed in one specimen. Done both diagnostic and therapeutic in most cancer types. Which nodes are removed depend on the location of the cancer. But this was the first node dissection I’d filmed for melanoma and that made it interesting. In most cancer types metastatic lymph nodes are just enlarged. But in melanoma they turn dark. I guess it must be because of the pigment produced by the cancerous melanocytes.
At first this was not visible, but after the specimen was removed and several nodes cut open, almost black tissue could be seen.

By the end of the day I’d seen and learned something completely different than I expected when sitting on the tube to work. I like it when workdays are hectic and a bit unpredictable.

I like it when workdays are hectic and a bit unpredictable.
Which is exactly (one reason) why I love trauma!
I’ve never been present at emergency surgery, but I can imagine it must be challenging.
Finding solutions as you go to unexpected problems.
Filming trauma care on the other hand…”Keep him awake! Do you hear me, sir? I need you to sign…We need your consent to…Ah, too late.” ;)
[…] out at The Sterile Eye, a blog by a medical videographer. (via Suture for a […]
[…] have written about the filming of this third video before. It is a left inguinal lymph node dissection on a patient with malignant melanoma. I was deeply […]
[…] video was recorded in February, and I wrote a post about the experience then. I’ve pasted the description of the operation […]